The GLP-1 market has been rewritten twice in three years, first by semaglutide, then by tirzepatide, and most of the buyer’s guides floating around online still read like it’s 2023. Liraglutide, the original approved GLP-1 weight-loss injection, got quietly reclassified in that process. It isn’t the headline drug anymore. It also isn’t obsolete, expired, or a scam, and a surprising number of pages online can’t seem to hold both of those facts at once.
Here’s the state of play as of this review.
The backstory, fast
Liraglutide is a lab-built copy of a hormone your gut releases after a meal. That hormone tells your pancreas to release insulin when blood sugar climbs, slows stomach emptying, and flips a switch in the brain that says “you’re full.” The natural hormone breaks down in minutes. Liraglutide was engineered to last long enough that a once-daily shot keeps the fullness signal running.
Two brand names, one molecule, two different jobs. At lower doses it’s Victoza, cleared for type 2 diabetes. At 3 mg daily, it’s Saxenda, cleared specifically for chronic weight management alongside diet and exercise changes. The FDA approved Saxenda for adults, then extended that approval down to adolescents age 12 and up with obesity [1][2]. That’s a real, documented approval record, not marketing copy.
One operational detail matters more than people expect: this drug is a daily injection, not weekly. That single fact is the reason a lot of people quit before they see results.
The numbers, unfiltered
In the pivotal SCALE Obesity and Prediabetes trial, adults without diabetes lost about 7.9 percent of body weight on liraglutide 3 mg over 56 weeks, versus about 2.6 percent on placebo. Roughly 63 percent of the drug group hit at least 5 percent weight loss, against about 27 percent on placebo [3]. In people with type 2 diabetes, where weight loss is typically harder, the SCALE Diabetes trial recorded about 6 percent loss on liraglutide versus about 2 percent on placebo [4].
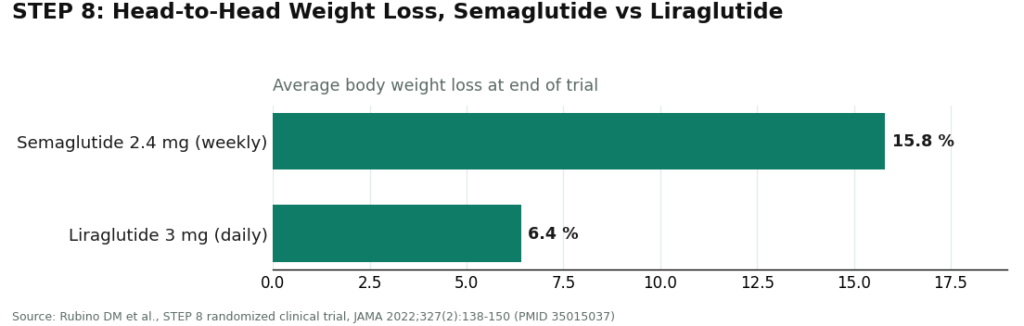
Those are legitimate, clinically meaningful results. They are also no longer the best numbers in the room. The STEP 8 trial put semaglutide and liraglutide head-to-head, and once-weekly semaglutide 2.4 mg produced about 15.8 percent average weight loss compared with 6.4 percent on once-daily liraglutide 3 mg [6]. That gap is the entire reason liraglutide’s market position shifted. Tirzepatide posts bigger numbers still, in its own separate trials.
But liraglutide holds one card the newer drugs are still building their own version of. In the LEADER trial, in people with type 2 diabetes at high cardiovascular risk, liraglutide cut the combined rate of cardiovascular death, nonfatal heart attack, and nonfatal stroke, hazard ratio 0.87 [5]. That’s a measured outcome in real cardiac events, not a stand-in lab marker. For a specific slice of patients, that’s a documented reason a clinician might reach for this drug on purpose, not out of habit.
What it means for someone deciding today
Bottom line for anyone shopping this category in 2026: if maximum weight loss is the only variable, semaglutide or tirzepatide will generally outperform liraglutide, and nobody being straight with you will pretend otherwise. Liraglutide still earns its spot for specific reasons: the LEADER cardiovascular data [5], the longest real-world track record of any modern GLP-1 simply from time on the market, approval down to age 12 [2], and its usefulness when the weekly drugs are backordered. Those are legitimate reasons to choose it. “It was cheaper on the site I found first” is not.
The three doors, ranked
Reporting on this space keeps turning up the same structural problem: three ways to get liraglutide, only two of them defensible.
Door one: branded Saxenda or Victoza from a licensed retail pharmacy with a prescription. Straightforward, regulated, no ambiguity.
Door two: compounded liraglutide from a licensed compounding pharmacy, prescribed and monitored by a clinician. Legitimate, provided the oversight is real.
Door three: unlabeled “research use only” powder or vials, no clinician, no prescription, no accountability for what’s actually in the vial. Walk past this one.
The reason door three is dangerous isn’t abstract. Liraglutide requires a slow, staged dose climb, not a jump straight to 3 mg. Skip the titration and the nausea, vomiting, and diarrhea this drug class is known for tend to spike hard enough that people quit outright, which is exactly what the FDA label’s titration schedule is built to prevent [1]. In the adolescent trial, gastrointestinal side effects ran clearly higher than placebo, and a real share of teenagers stopped the drug because of them [7]. An unlabeled seller offers zero titration guidance, zero monitoring, and conveniently skips the label’s boxed warning on thyroid C-cell tumors seen in rodent studies and the contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 syndrome [1]. “Research use only” isn’t a technicality. It’s how the seller avoids ever being on the hook for what happens next.
For anyone going the supervised route, the model worth understanding is how a physician-led telehealth service such as FormBlends actually runs the process: a clinician reviews the patient’s history before anything ships, a licensed pharmacy fills the prescription rather than a lab-labeled supplier, and someone tracks the dose climb and follow-up check-ins over the months that determine whether the drug actually works for that person. That structure isn’t an add-on fee dressed up as care. On a drug with a real contraindication list and a titration schedule that decides tolerability, the supervision is most of what’s actually being purchased. The compound itself is cheap and available everywhere. Nobody’s discounting the oversight.
Quick answers
Is it actually FDA approved? Yes. Saxenda is approved for chronic weight management alongside diet and exercise, and the same molecule at lower doses, Victoza, is approved for type 2 diabetes [1][2]. Compounded liraglutide is a different regulatory category from the approved branded product, and any provider worth using will say so unprompted.
Does it keep up with semaglutide and tirzepatide? Not on weight loss specifically. STEP 8 put it at roughly 15.8 percent for semaglutide against 6.4 percent for liraglutide [6]. It still delivers real, documented weight loss [3], just not the category-leading numbers anymore.
So why would anyone still pick it? The LEADER cardiovascular data [5], the longer safety track record from years on the market, approval down to age 12 [2], and availability during stretches when the weekly drugs are hard to source. Whether any of that applies to a given patient is a clinician’s call, not a guess made from a headline.
What’s the trade-off? Daily injections instead of weekly, gastrointestinal side effects concentrated during the dose climb, and a label carrying real warnings [1][7]. None of that makes it a bad drug. It makes it a drug that needs a clinician in the loop, not a comment-section recommendation.
The takeaway
Liraglutide’s story in 2026 is not a scandal and not a miracle, it’s a market correction. It’s approved, it’s been studied for a decade-plus, it carries a genuine cardiovascular benefit and the longest safety record in its class, and it’s also been passed by newer weekly drugs on pure weight-loss numbers. All of that is true simultaneously. The real risk was never the molecule. It’s buying it from an unlabeled vial with no clinician watching the dose, and that risk is entirely avoidable.
References
- U.S. Food and Drug Administration. Saxenda (liraglutide injection 3 mg) prescribing information, including boxed warning on thyroid C-cell tumors and dose titration schedule. Accessdata FDA. https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/206321s011lbl.pdf
- U.S. Food and Drug Administration. FDA approves weight management drug for patients aged 12 and older (Saxenda), December 4, 2020. https://www.fda.gov/news-events/press-announcements/fda-approves-weight-management-drug-patients-aged-12-and-older
- Pi-Sunyer X, Astrup A, Fujioka K, et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management (SCALE Obesity and Prediabetes). New England Journal of Medicine. 2015;373(1):11-22.
- Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide for weight loss among patients with type 2 diabetes: the SCALE Diabetes randomized clinical trial. JAMA. 2015;314(7):687-699.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes (LEADER). New England Journal of Medicine. 2016;375(4):311-322.
- Rubino DM, Greenway FL, Khalid U, et al. Effect of weekly subcutaneous semaglutide vs daily liraglutide on body weight in adults with overweight or obesity without diabetes: the STEP 8 randomized clinical trial. JAMA. 2022;327(2):138-150.
- Kelly AS, Auerbach P, Barrientos-Perez M, et al. A randomized, controlled trial of liraglutide for adolescents with obesity. New England Journal of Medicine. 2020;382(22):2117-2128.